Trauma and Resilience-Informed Care

Action Steps Using ACEs and Trauma-Informed Care: A Resilience Model
This paper 1) discusses two important contributions that are shaping work with vulnerable and under-resourced populations: Kaiser Permanente’s (1998) Adverse Childhood Experiences Study (ACE) which includes the impact of adverse experiences in childhood on adult health and health behaviors and the more recent advent of what has come to be known as Trauma-Informed Care (TIC), programs which incorporate knowledge of the impact of early trauma into policies and programs. 2) Despite many positive benefits that have come from both contributions there are unintended consequences, described in the paper, that have an impact on research and program evaluation as well as social policies and programs. 3) Three key neuroscience concepts are recommended for inclusion in Trauma-Informed Care programs and practices in ways that can enrich program design and guide the development of practical, resilience-oriented interventions that can be evaluated for outcomes. 4) Finally, a resilience-oriented approach to TIC is recommended that moves from trauma information to neuroscience-based action with practical skills to build greater capacity for self-regulation and self-care in both service providers and clients. Examples from criminal justice are used.

Positive and Adverse Childhood Experiences Survey (PACES), 2015: An Alternative to the ACE Survey
PACES (Positive and Adverse Childhood Experiences Survey) is a brief questionnaire designed as an alternative to the ACE Survey. It includes questions about protective factors. These protective-factor questions are interspersed with the items from the ACE Survey in a way that can help to decrease the potential for re-traumatization, maintain a balance between activating and calming questions, and help provide a richer understanding of early childhood experiences.
PACES was developed to highlight the importance of understanding positive as well as adverse events in shaping a variety of outcomes and also to demonstrate how questionnaire construction can be used in a way that reduces the likelihood of re-traumatization and help maintain the research individual in a “Zone of Resilience” and not of dysregulation when answering questions. PACES has two key components that differentiate it from the ACE Survey: 1. Questions that collect positive childhood events in addition to adverse events and 2) the interspersing of protective questions that allow for a rhythm of questioning that moves between activating and calming questions in a way that mirrors the rhythm of the Autonomic Nervous System when it is in the Resilient Zone. In this zone of functioning individuals are more likely to have a clear memory and thought processes.
The Biology of Resilience
The Nervous System and Resilience
The term “mental health” is outmoded. We know that the mind and body are a system, inseparably connected; so we really need a term that reflects interventions that explicitly work with both. Candace Pert has called this “bodymind,” others refer to “holistic” or “integrative” models. The fact that there is not a term that is universally used and understood reflects the fact that this is a relatively new frontier for psychotherapists and other clinicians and practitioners. Regardless of the term that eventually is used, SRM is a model that works to connect and heal the bodymind system… from the inside-out.
The goal in this essay is to provide current neuroscience information that is relevant for work with others and for practitioner self-care. There is a vast and growing body of information about the human nervous system. The goal in this essay is to provide the information that helps you understand why it is so important to work with the nervous system and how SRM skills can amplify stability and resilience across stress-spectrum disorders as well as for self-care.
The Missing Link: The Biology of Human Resilience
In the face of so much turbulence and calamity in the world is it any wonder why for the past 50 years we have increasingly looked to the concept of resilience to guide us in understanding how to create a world in which all are safe, fed, housed, and nourished? Much has been written about resilience and increasingly we are seeing creative, determined,and often successful efforts implemented which bring the core concepts into action in behalf of planetary suffering; applying evidence-based approaches to rescuing and restoring the environment, rebuilding communities destroyed by natural and human-caused disasters, and strengthening the opportunities for poor and vulnerable populations.
There are several of us at the Bellagio Center whose work is focused on Resilience. And we know the Rockefeller Foundation is holding a conference on the topic on April 19. This essay is our effort to contribute a new but essential link to the discussion, the neurobiology of human resilience.

Vulnerable Populations
Information Gathering After Trauma: Considerations for Human Rights Work, Peacebuilding, and Interviewing
The collection of information from victims of human cruelty, as well as survivors of natural disasters, can provide essential information for use in promoting justice, enhancing peace building, and developing preventive programs. Victims and interviewers often believe that telling the story of what has happened will not only provide needed evidence, but also represents the beginning of healing. Today neuroscience can contribute positively to the way that traumatic-events evidence is collected. The way that someone’s story is told has a powerful impact on whether the interview or debriefing process will be re-traumatizing to the victim (or survivor) or will be a step toward healing and will promote or reduce the likelihood of secondary traumatization for the interviewer. The trauma resiliency model for collecting evidence seeks to manage high arousal,contribute to the healing and resiliency of survivors, and reduce potential secondary traumatization and burnout by interviewers.

Domestic Minor Sex Trafficking: Identifying and Responding to America’s Prostituted Youth
Traumatic events have a profound effect, not only on a victim’s psychological state, but also their neurological and physical states. The behaviors shown by domestically trafficked minors that are often bewildering and frustrating for first responders, such as running away, unclear or disjointed memories, trauma bonding, aggression, etc., are symptomatic of biological processes that occur when chronic traumatic experiences occur in a young person’s life.
Available for purchase from sharedhope.org
It Takes A Community
The debate about our involvement in Iraq and Afghanistan has raged for a decade, but no one disputes one fact: as a result of those conflicts, thousands and thousands of young men and women have been profoundly wounded – physically, emotionally, and spiritually. The statistics measuring the effects of wartime service on our troops reveal high rates of drug and alcohol abuse, homelessness, homicide, suicide, divorce, depression, traumatic brain injury, and post-traumatic stress disorder. Yet, unless we’re closely related to someone in the military, many of us still feel insulated from the impact of these wars, detached from the sacrifices of those fighting them, and removed from the problems they experience only once they return to civilian life.
Projects in Post-Conflict Countries

Somatic Approaches and Peacebuilding
Inclusion of a somatic approach in post-conflict societies as a component for increased inclination to peacebuilding and reconciliation: preliminary evidence from the field: Contemporary neuroscience research has shed important light on the way the mind- body system responds to threat and fear. As a result, somatic approaches that build on neuroscience research are now gaining visibility as they offer practical ways for individuals and communities to self-regulate following traumatic events.
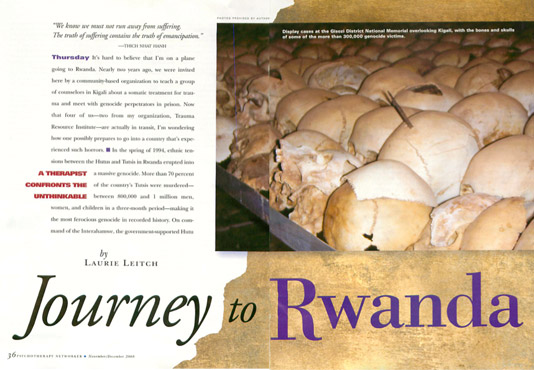
Journey to Rwanda
It’s hard to believe that I’m on a plane going to Rwanda. Nearly two years ago, we were invited here by a community-based organization to teach a group of counselors in Kigali about a somatic treatment for trauma and meet with genocide perpetrators in prison. Now that four of us – two from my organization, Trauma Resource Institute – are actually in transit, I’m wondering how one possibly prepares to go into a country that’s experienced such horrors.
The Rwanda Baseline Study: Preliminary Findings and Recommendations
Limited data exists that provides an understanding of the strengths and challenges of the génocidaires incarcerated in Rwandan prisons following the 1994 genocide. Understanding the strengths of génocidaires and the challenges they face can help prepare incarcerated génocidaires for healthy reentry into their communities. Such data provides:
- A better knowledge about how to build on the existing strengths of génocidaires during their remaining time in prison and after their release;
- A better understanding of the kinds of supportive activities and services that are needed to address the challenges and vulnerabilities of the génocidaires during their remaining time in prison and after their release;
- An increased likelihood for public and private organizations to use the data to collaborate on more comprehensive and coherent approaches, which strengthen the social fabric of communities;
- Reduction of recidivism by designing services that are sensitive to both the needs and strengths of those leaving prison and their communities.
Recovery After Genocide: Understanding the Dimensions of Recovery Capital Among Incarcerated Genocide Perpetrators in Rwanda
Utilizing survey data from 302 men and women incarcerated in the Rwandan correctional system for the crime of genocide, and structured interviews with 75 prisoners, this mixed methods study draws on the concept of recovery capital to understand how individuals convicted of genocide navigate post-genocide healing. Genocide smashes physical and human capital and perverts social and cultural capital. Experiencing high levels of post traumatic stress symptoms with more than two-thirds of the sample scoring above typical civilian cut-off levels, raised levels of depression, and high levels of anxiety, and failing physical health, the genocide perpetrators require multiple sources of recovery capital to foster internal resilience as they look forward to rebuilding their own lives.
Reconciliation potential of Rwandans convicted of genocide
This study examines the reconciliation potential of Rwandans incarcerated for the crime of genocide. Utilising survey data from 302 male and female prisoners incarcerated in the Rwandan Correctional System, this study explores genocide perpetrators’ depression, anxiety, anger-hostility and somatic symptoms, levels of post‐traumatic stress, degree of social support and attitudes towards unity and reconciliation. The data demonstrate that engaging in killing can have deep psychological impacts for genocide perpetrators. The data indicate that although more than two decades have passed since the genocide, perpetrators are experiencing high levels of genocide-related post-traumatic suffering. Perpetrators are persistently re-experiencing genocide, purposefully avoiding thoughts and memories of the genocide, and experiencing physical and emotional arousal and reactivity. The sample had a strong desire for all Rwandans to live in peace and unity. There is, however, an urgent need for physical and mental health interventions, as well as services that facilitate the rebuilding of family relationships well in advance of release. Improving the physical and mental well-being of both perpetrators of the genocide and victims can only be a positive development as Rwanda continues to build a unified, reconciled and resilient future.
Natural Disasters
Somatic Experiencing Treatment With Tsunami Survivors in Thailand: Broadening the Scope Of Early Intervention
This exploratory study examines the treatment effects of brief (1 to 2 sessions) Somatic Experiencing with 53adult and child survivors of the 2004 tsunami in Thailand. Somatic Experiencing’s early-intervention model, now called Trauma First Aide, was provided1 month after the tsunami. Survivor assessments were done pretreatment, immediately posttreatment, 3 to5 days posttreatment, and at the 1-year follow-up.Results indicate that immediately following treatment,67% of participants had partial to complete improvement in reported symptoms and 95% had complete or partial improvement in observed symptoms. At the 1-yearfollow-up, 90% of participants had complete or partial improvement in reported symptoms, and 96% had complete or partial improvement in initially observed symptoms. Given the small sample size and lack of an equivalent comparison group, results must be interpreted with caution. Nonetheless, the results suggest that integrative mind–body interventions have promise in disaster treatment.
A Case for Using Biologically-Based Mental Health Intervention in Post-Earthquake China: Evaluation of Training in the Trauma Resiliency Model
Catastrophic events, such as the Sichuan Province earthquake in China on May 12, 2008, cause massive suffering. They put a huge strain on local response capacities because of distress of the civilian population and also death and traumatization of local responders. Mental health approaches are needed that are efficient and that help provide stabilization to both responders and civilians. The article has two goals: First, to present a rationale for the use of a biologically-based model of mental health, the Trauma Resiliency Model (TRM), in post-disaster settings and, second, to present evaluation results of TRM training, mental health training focused on the biology of threat and fear with corresponding treatment skills provided as part of the China Earthquake Relief Project (CHERP). TRM training was provided to a non-random sample of more than 350 doctors, nurses, teachers, and counselors during a 18 month period after the earthquake. TRM training was provided in six cities to expand local response capacity by providing didactic sessions and practice in TRM’s trauma treatment skills. CHERP’s focus on acquisition of practical treatment skills and local sustainability provided TRM skills refresher training sessions over the entire course of the project. The Training Relevance, Use, and Satisfaction Scale(TRUSS) and the Training Evaluation Form (TEF) were used throughout the months of training and supervised practice. Results indicate 97% believe that biologically-oriented TRM training will be very to moderately relevant or useful for their work with the Chinese earthquake survivors, and about 88% report they will use the skills very to moderately frequently during the two weeks following the training. Over 60% of the trainees report they will use TRM skills for their own self-care.

Somatic Experiencing Treatment with Social Service Workers Following Hurricanes Katrina and Rita
In a disaster, social service workers are often survivors themselves. This study examines whether somatic intervention using a brief (one to two session) stabilization model now called the Trauma Resiliency Model™ (TRM), which uses the skills of Somatic Experiencing® (SE), can reduce the postdisaster symptoms of social service workers involved in postdisaster service delivery. The study was implemented with a nonrandom sample of 142 social service workers who were survivors of Hurricanes Katrina and Rita in New Orleans and Baton Rouge, Louisiana, two to three months after the disasters. Ninety-one participants received SE/TRM and were compared with a matched comparison group of 51 participants through the use of propensity score matching. All participants first received group psychoeducation. Results support the benefits of the brief intervention inspired by SE. The treatment group showed statistically significant gains in resiliency indicators and decreases in post traumatic stress disorder symptoms. Although psychological symptoms increased in both groups at the three to four month follow-up, the treatment group’s psychological symptoms were statistically lower than those of the comparison group.
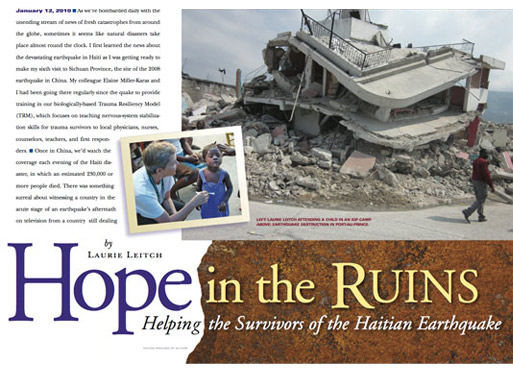
Hope in the Ruins: Helping the Survivors of the Haitian Earthquake
As we’re bombarded daily with the unending stream of news of fresh catastrophes from around the globe, sometimes it seems like natural disasters take place almost round the clock. I first learned the news about the devastating earthquake in Haiti as I was getting ready to make my sixth visit to Sichuan Province, the site of the 2008 earthquake in China. My colleague Elaine Miller-Karas and I had been going there regularly since the quake to provide training in our biologically-based Trauma Resiliency Model (TRM), which focuses on teaching nervous-system stabilization skills for trauma survivors to local physicians, nurses,counselors, teachers, and first responders.